

Protein Recommendations Are a Moving Target: How to Actually Assess Adult Needs
by Bridget Storm MA, RD-AP, LDN, CNSC
Protein needs in adults are more nuanced than a single number. This post reviews major protein recommendations, where they come from, and how to apply them in practice, with a balanced look at the strengths and limitations of the evidence.
The RDA: A Starting Point, Not a Prescription
The Recommended Dietary Allowance (RDA) for protein is 0.8 g/kg/day for adults. This value is designed to meet the needs of nearly all healthy individuals and prevent deficiency under typical conditions, not to define an “optimal” intake for every situation.
Key assumptions behind the RDA include:
The individual is generally healthy.
Energy intake is adequate, so protein is not diverted to meet energy needs.
There is no major metabolic stress (e.g., acute illness, trauma, surgery).
In other words, 0.8 g/kg/day is a population-level minimum requirement, not a personalized target for all adults across all settings.
National dietary surveys, including data from What We Eat in America (WWEIA), NHANES 2015–2016, suggest that average U.S. adults consume protein at or above this level, often around 1.0 g/kg/day and contributing roughly 14–16% of energy intake. These surveys indicate that most adults meet or exceed the RDA without deliberate protein-focused strategies.
2026 Dietary Guidelines: Higher Targets, Weak Foundations
Recent Dietary Guidelines for Americans (DGA) discussions and advisory materials have highlighted higher protein intakes—often cited in the range of approximately 1.2–1.6 g/kg/day for some adults, especially older adults and those focused on preservation of lean mass and metabolic health.
There are reasonable scientific motivations for considering higher intakes in selected groups: higher protein may support maintenance of lean body mass when combined with resistance exercise, may promote satiety, and may help attenuate age‑related muscle loss in older adults.
However, the evidence base is not uniform, and it is important to present these recommendations with appropriate caution:
Many trials are relatively short in duration, use tightly controlled conditions, or focus on surrogate outcomes (e.g., lean mass, nitrogen balance) rather than long‑term clinical endpoints such as physical disability, hospitalization, or mortality.
Studies differ in population characteristics, baseline diets, and intervention designs, which makes it challenging to define a single “ideal” protein range applicable to all adults.
Observational analyses suggest nonlinear associations between protein intake and outcomes (such as all‑cause mortality), with risk sometimes increasing at both very low and very high intakes, particularly above roughly 1.3–1.5 g/kg/day in some subgroups.
Taken together, higher protein targets in the 1.2–1.6 g/kg/day range can be viewed as emerging, context‑specific recommendations that may benefit certain populations (for example, physically active adults or older adults at risk of sarcopenia), rather than as definitive population‑wide goals.
Older Adults: A Targeted Increase
With aging, anabolic resistance, chronic disease burden, and functional decline increase the risk of sarcopenia and frailty. For older adults, protein intakes above the general adult RDA are recommended.
Recent ASPEN‑aligned recommendations suggest approximately 1.0–1.3 g/kg/day for many older adults, with the exact target individualized based on health status, comorbidities, and goals of care.
This range strikes a middle ground:
Higher than the RDA to support muscle maintenance
More conservative than emerging high-protein proposals
Flexible enough to individualize based on function, comorbidities, and intake
At the same time, these recommendations emphasize clinical judgment. Conditions such as advanced chronic kidney disease, severe frailty, or very limited oral intake may warrant careful balancing of potential benefits and risks when setting protein targets
Critical Increases for Critical Illness
Critical illness creates a markedly different metabolic environment from community‑dwelling health. Inflammation, hormonal changes, and immobilization increase protein catabolism and lean body mass loss.
Major critical care nutrition guidelines generally recommend protein intakes in the range of 1.5–2.0 g/kg/day for most critically ill adults, adjusted for factors such as obesity, renal function, and tolerance. These recommendations are largely supported by nitrogen balance studies, observational data, and expert consensus indicating that protein requirements are substantially higher in critical illness than in health.
At the same time, higher prescribed protein does not consistently translate into improved hard outcomes (such as mortality or ICU length of stay) across all studies, underscoring the complexity of critical illness and the difficulty of isolating the effect of protein dose from other aspects of care. The EFFORT study (Heyland et al. 2023) suggested a potential dose-dependent harm with high amounts of protein (> 1.8 g/kg) early in critically ill patients with AKI & high organ failure scores, but most EN formulas do not reach such high doses without overfeeding total kcal. Practical barriers such as feeding intolerance, interruptions to nutrition support, and varying degrees of anabolic resistance also influence how much protein can be delivered and utilized.
Using guideline ranges as a starting point and individualizing based on clinical course, organ function, and feeding tolerance reflects a balanced approach.
Putting Protein Recommendations into Practice
In everyday practice, many registered dietitians estimate protein needs for generally healthy adults around 1.0 g/kg/day, based on clinical judgment. This “middle‑ground” target:
Provides a modest buffer above the 0.8 g/kg/day minimum while avoiding very high intakes by default.
Often aligns with typical observed intakes in many adults, based on NHANES data.
Offers a simple starting point that can be adjusted upward or downward for factors such as physical activity, early rehabilitation, mild illness, or specific patient goals.
Protein needs are not static; they depend on health status, age, metabolic stress, and overall intake.
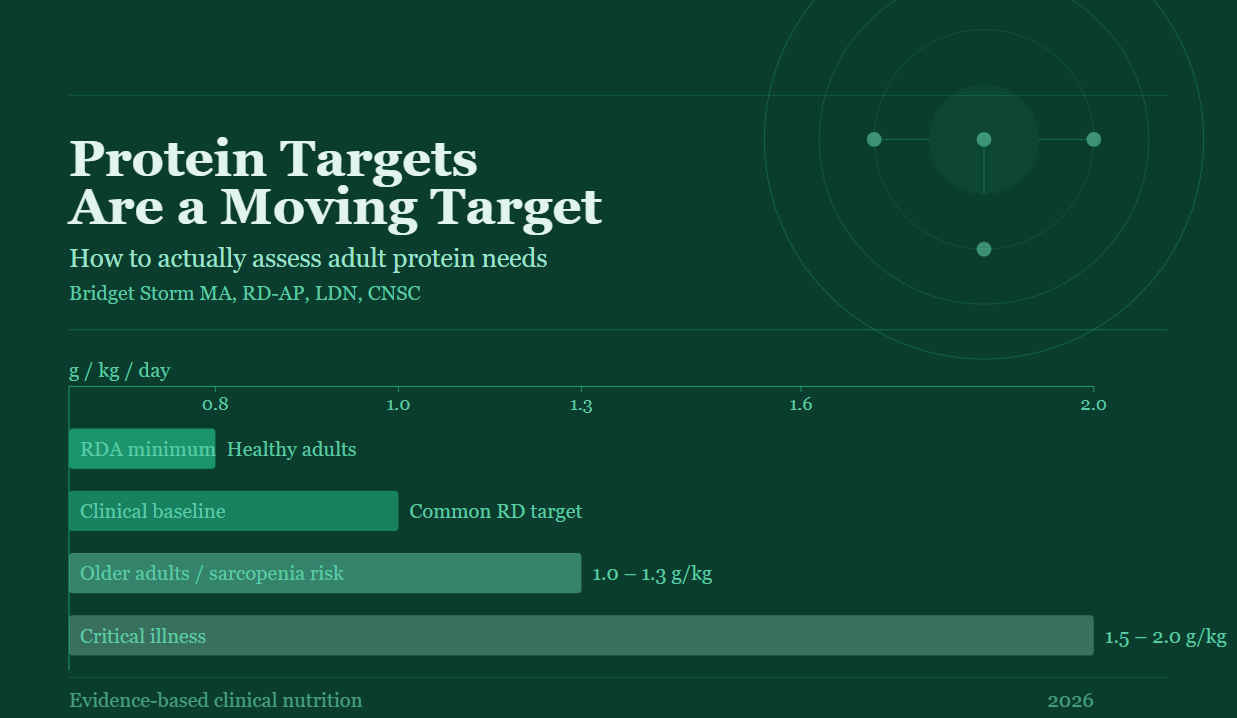
A practical framework:
0.8 g/kg/day: Minimum requirement for healthy adults
~1.0 g/kg/day: Common clinical baseline
1.0–1.3 g/kg/day: Older adults or those at risk of muscle loss
1.5–2.0 g/kg/day: Critical illness
Rather than chasing a single “optimal” number, clinicians should focus on individualized assessment and remain cautious about adopting higher targets that outpace the evidence.
References:
American Heart Association. Protein: What’s Enough? Updated 2024. Accessed April 2026. https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/nutrition-basics/protein-and-heart-health.
Hoy MK, Clemens JC, Moshfegh A. Protein Intake of Adults: What We Eat in America, NHANES 2015-2016. Beltsville (MD): United States Department of Agriculture (USDA); Available from: https://www.ncbi.nlm.nih.gov/books/NBK589212/
Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey (NHANES). Accessed April 2026. https://www.cdc.gov/nchs/nhanes/index.html.
U.S. Department of Agriculture, U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025. www.dietaryguidelines.gov.
U.S. Department of Agriculture, U.S. Department of Health and Human Services. Data Analysis for the 2025 Dietary Guidelines Advisory Committee Report. https://www.dietaryguidelines.gov/2025-advisory-committee-report/data-analysis.
National Council on Aging. How Much Protein Do Older Adults Need? 2025. Accessed April 2026. https://www.ncoa.org/article/how-much-protein-do-older-adults-need/.
Tao X, Yi Y, Yang Y, Zhao Z. Association between dietary protein intake and all-cause mortality among individuals with different estimated glomerular filtration rates: A cohort study from NHANES. Medicine (Baltimore). 2025;104(52):e45670. doi:10.1097/MD.0000000000045670.
Chan, LN, et al (Eds). The ASPEN Adult Nutrition Support Core Curriculum, 4th Edition. ASPEN 2025.
Compher C, Bingham AL, McCall M, et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: the American Society for Parenteral and Enteral Nutrition. JPEN. 2022; 1-30. https://doi.org/10.1002/jpen.2267.
McClave, SA et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN. 2016: 40 (2): 159-211. http://sccmmedia.sccm.org/documents/LearnICU/Guidelines/Nutrition-SCCM-ASPEN.pdf.
Heyland DK, Patel J, Compher C, et al; EFFORT Protein Trial Investigators. The effect of higher protein dosing in critically ill patients with high nutritional risk (EFFORT Protein): an international, multicentre, pragmatic, registry-based randomised trial. Lancet. 2023;401(10376):568-576. doi:10.1016/S0140-6736(22)02469-2.
CDC. Dietary Data – Continuous NHANES. Accessed April 2026. https://wwwn.cdc.gov/nchs/nhanes/.